
Developing Aortic Stenosis due to a Bicuspid Aortic Valve
This is one doctor’s experience as an explainer to friends, family and anyone who has a bicuspid aortic valve or who, for whatever reason, has developed Aortic Stenosis.
Early days
I was born half way through 1967. My mother was barely 27. She had qualified as a teacher before embarking on a family and was an older mum compared to many of her peers at that time. I was her first. As the world looked up to the stars, then still anticipating man walking on the moon, my mother was told that “I would never be an astronaut”. Her beautiful baby had a heart murmur – some sort of defect which meant, according to the doctors, that I would never be fit enough to get into space.
Heart murmurs
In truth, that limitation of my career trajectory may have been quite unnecessary. A heart murmur is merely the noise blood makes flowing through the heart. It’s an audible ripple from the eddies blood makes as it’s being pumped from one chamber of the heart to the next, and out to the body. Murmurs may signify there’s ‘a problem’ with the heart. Normally, blood flows through the heart almost silently. Doctors can hear the valves opening and closing and hopefully not much else. Many heart murmurs, heard soon after birth, disappear with age and all babies should be re-examined at 6-8 weeks of age to see if they’ve gone. Many are just innocent ‘flow’ murmurs and nowadays would be investigated further if they persist. Some can be due to physiological changes that occur soon after birth and these go within days, others can be due to major heart abnormalities, some of which, if it weren’t for modern medicine, wouldn’t be compatible with life, though usually the blue colour of the baby makes that fairly obvious. I was pink, – albeit whingy – and my problem was not, at that point, serious.
In 1967 there wasn’t the technology for readily seeing inside the heart. X-rays with dye might show some, but not all abnormalities. Heart murmurs in otherwise pink and feeding babies were deemed not to be overly important. My mother just had to accept that, if she had ever had ambitions for me to become an astronaut, they were not to be. I clearly remember her telling me several times that, I wouldn’t be able to become an astronaut, as if I was missing a limb!
Diagnosis
Eighteen years later she wasn’t too disappointed though to see me get into medical school and during the undergraduate course grab an opportunity to go and work with the Royal Flying Doctor Service in outback Australia. The Australian visa necessary for such an adventure required a full medical with my university GP. He was clinically astute. He heard the murmur, still there at the ripe old age of 21, predicted it was due to a congenital abnormality called a bicuspid aortic valve and referred me to a favourite lecturer, Professor David Wood, for confirmation.
By the mid-1980s the National Health Service in the UK had echocardiography. Using this ultrasound wizardry Prof. Wood confirmed a bicuspid aortic valve. By this time, I’d looked the condition up in the hefty pathology tome I owned. It affects 1% of the population and is hereditary in a small proportion, so if you have it, ensure your siblings and children are screened for it, and your parents, if they’re still around, when you discover it. It doesn’t normally impact on life until the fifth or sixth decade, and the impact then, if you’re unlucky, can be sudden and final, though for many they get warning symptoms that need good clinicians to note and diagnose.
What is it and what does it matter?
A normal aortic valve looks, if you’re looking down on it, like the Mercedes symbol. There are three flaps to it that open and close with every heartbeat. A bit like a three petalled flower, opening and closing with daylight, but a lot faster! A bicuspid valve only has two flaps, something like a circle with a line across it. The line is just the gap though through which blood flows. It’s not dissimilar to a goldfish opening and closing its mouth.
The trouble with only two flaps is they have to do the work of three and over time they wear faster. They get calcified, and stiff and they restrict the flow of blood from the left ventricle of the heart into the aorta. That restriction is called Aortic Stenosis. From here it should flow freely to the rest of the body. Restricting heart flow is never good. The muscle of the left ventricle gets beefed up to try and overcome the restriction and that makes it vulnerable to problems with its electrical system. Left ventricular muscle beefing up is called hypertrophy. It’s a process that takes time, years if not decades, and if unchecked it is a cause of many sudden deaths from abnormalities in electrical conduction and then rapid disorganised contraction of the heart muscle. That ain’t good! In truth, it’s so bad it leads to collapse and often a quick demise.

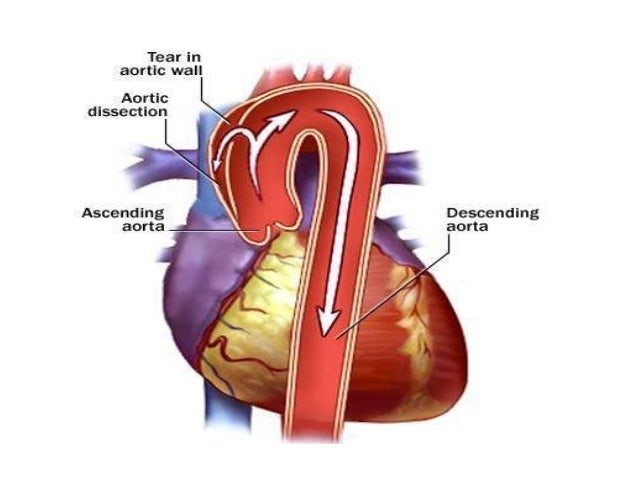
If that mode of death doesn’t get the hapless folk with an undiagnosed bicuspid valve the widening of the aorta, the big blood vessel that comes out of the heart and leads the blood around the entire body may similarly cause an abrupt ‘game over’. The aorta stretches with each pulse of blood coming out of the heart, sixty or eight times a minute, or 150 times a minute if you’re an athlete working hard. The aorta of someone with a bicuspid valve probably tries to compensate for the restricted flow through the valve by lowering the resistance beyond, and getting wider, but weaker.
Doctors call this dilatation and it leaves the aorta vulnerable to tears, that are known as aortic dissection. When the aorta in the chest tears, the window of opportunity to fix it is pretty small, depending on the extent and speed of the tear. If you’re standing outside a cardiothoracic operating theatre, you have a better chance than the majority who will be miles away living their lives. That said, it is survival for those who get to a hospital capable of treating it, and not all are. The symptoms are interscapular (between the shoulder blades) pain, often described as ripping, which comes on suddenly abruptly. If you know you’re at risk just dial 999 (or 112) if you get it and tell them you think you might have an aortic dissection!
The good news for the patient is the mode of death is pretty quick compared to the lingering deaths of aggressive cancer or dementia. For arrhythmias it might be minutes. For dissections it’s a few hours. For those around them it’s awful. They might have to do CPR and try to resuscitate you. It’s worth them learning how to do this, but you and they have to be realistic. The chances of survival are slim. Pathology and physiology just aren’t on your side.
For these very justifiable reasons anyone with a bicuspid aortic valve should have monitoring echocardiograms done regularly. The interval can be 3-5 years when you’re young and annually or less as the valve is seen to stiffen, the ventricle muscle gets beefier or the aorta dilates. All of this is readily measurable with today’s high tech. The pressure difference across the valve can be measured too. I knew my numbers over the years were deteriorating – I’d kept them all. I knew I already had some ventricular hypertrophy, (the thickening of the heart muscle) and the pressure gradient across the valve was increasing. It had reached 50mmHg a couple of years previously. This is classed as moderate stenosis – i.e. moderate restriction of the blood flow out of the heart. Although I knew all this I had never really given the consequences much thought. I had kept pretty fit during my adult life and hadn’t really given any thought about the day things got really bad nor had I realised I was symptomatic of a deterioration. It’s difficult to be objective about symptoms that come on gradually, particularly if you’re a doctor, and especially if you’re a bloke! Perhaps that’s why so many seem to die suddenly around the age of retirement, for all sorts of reasons.

My story
I have been having regular checks for years. In recent years the interval had dropped from every 3 years to every twelve, and then, nine months. In March 2023 I was off-piste skiing, doing what I love, skiing ‘steep and deep’ powder, through trees around Chamonix. My fitness in recent years has not been what it was ten years ago and I was feeling it. Blowing my own trumpet to the max, I was told that the ski instructor leading us (a former Olympic skier herself) judged me to be an advanced skier, (a ‘purple’ for those familiar with Ski Club of Great Britain categories) if only I was fitter. Without the fitness I wasn’t ‘a purple’. I thought that was very fair. I know how to ski, but I just couldn’t find the physical effort needed to match the terrain. Each morning I felt drained and wondered whether I should go out and do it all again. I was enjoying it but I was disappointed with my lack of stamina. Videoing my step-sons doing a similar, if slightly easier pitch, a couple of weeks later my partner commented on my breathlessness, readily audible on the video, when I was standing still. I thought it was just the altitude and not being fit enough. Despite the boys having had less than two weeks of skiing under their belts, and highly annoyingly, becoming adept at off-piste so early into their skiing careers, I was having to work hard to keep up. But I still don’t think the had penny really dropped.
My partner had been commenting on my breathlessness at times for quite a while. I’d put that down to my asthma and had a few months before changed inhaler to see if that helped. I thought my asthma was better, but looking back, I was still becoming breathless after any little exertion.
I was due my annual echocardiogram whilst I was away skiing but the hospital had luckily rescheduled it for just after Easter. It was one of the first junior doctor strike days and I thought it would get cancelled but not needing junior doctors, it went ahead. Jane, the Chief Cardiac Physiologist had scanned me many times and asked how I was. I told her of my less than satisfactory stamina when skiing and she mused as she squeezed out the transducer gel “well perhaps the valve has got worse. Let’s see”.
Jane is very experienced and thorough. She normally takes about ten minutes to do the echo, take all the measurements and tell me the news. This time, it was the fastest echo I’ve ever had. Almost immediately Jane could see the narrowing was worse. The gradient was now 70mmHg and I needed something doing about it. She phoned Simon, a cardiologist colleague who had looked after me for years. Covering for striking juniors that day, he was in the hospital and able to come down to the department where we were. He’s a former cycling buddy and he told me straight: “Shaun, it’s now severe aortic stenosis. You need a new valve. I’ll refer you to the surgeons. Limit your heart rate”.
Six days later, I was in front of the surgeon. I’d never had an operation before, never had a general anaesthetic and here I was learning I urgently needed a new aortic valve. The operation involves splitting my sternum to open the chest, putting me on heart bypass, stopping my heart to be able to open it to put in a new metal valve, putting in some polyester based artificial artery, to replace the dilating aorta and then getting me off bypass, restarting my heart and sewing me up. It’s a 4 or 5-hour job. You wake up in Intensive Care with drips in your neck and arm, drain tubes coming out of your chest, a catheter and a wound over your breastbone. Privately it can costs anywhere from £50,000 to £100,000. Thank God we have the NHS in the UK.
The surgeon explained that I was under no obligation to have surgery although without it, I would probably die within the next two years. He said I had a fifty percent chance of dying within the next twelve months. If hip, hernia and cataract waiting lists had a similar mortality rate then tens of thousands would die before they got their op. Whilst there are fewer patients needing valve replacement there are also far fewer specialists who can perform this type of complex surgery. That said, there are still way too many cases for the NHS in its perilous post-austerity state to be able to fix quickly. Cardiac waiting lists had risen to a record high of 392,698 at the end of May 2023 in England. A third of these were waiting for longer than the NHS target of 18 weeks from identification of need for surgery for actual surgery[1]. Heart surgeons perform coronary artery bypass grafts and there are lots of patients that urgently need these.
From the prognosis risk I was given I quickly calculated that meant a cumulative 1% risk each week! Waiting three months – a standard NHS wait would give me a 1 in 8 chance of not making it. If I waited 6 months it would be double, a 1 in 4 chance of not making it. Friends in the profession reassured me that these risks were an overall risk for all types of patients, including some who were much older and frailer than I, so in truth my risks were lower but it was still pretty un-nerving.
The operation itself has a mortality (death) risk of 1% and a risk of a major stroke of 1%. For every hundred patients who have the surgery the chances are one will die during or soon after the procedure and one will have a major stroke and not fully recover. To me, that meant a 98% chance of pulling through well and then having a near normal life expectancy. I would have to take the drug warfarin, for the rest of my life, to anti-coagulate (thin) my blood and prevent small blood clots forming on the new metal valve. Blood clots can stop the metal valve opening properly or they can get detached and float off in the blood stream. They can cause strokes if they get lodged in small blood vessels in the brain, and damage anywhere else in the body, where they get wedged. Good warfarin management is a serious business.
The surgeon told me I was too young to have a bioprosthetic valve – from a pig or a cow – as these don’t last like metal ones do, and other surgical options, even though they wouldn’t need warfarin for ever were not recommended for me, as a relatively young patient. Warfarin itself creates a risk of dying from a haemorrhage, but that risk is only about 1% per year. That means of 100 patients who are all on warfarin one will die each year as a result of being on warfarin. It might be from a haemorrhagic stroke (a bleed in the brain) or from the stomach or bowel. A full 99 will live on, and those who do their own monitoring tend to have better control of the extent that their blood is thinned and be less likely to suffer such dire side effects of warfarin. I’ll never be able to binge on booze again but I don’t have to be teetotal.
I would be able to hear the valve ticking for ever but was told my brain would in time filter out the sound. For someone who has had a lifelong intolerance of ticking clocks, in the bedroom at least, that sounded to me like torture. The surgeon told me people sitting next to me wouldn’t be able to hear it so I wasn’t going to be looked at as if I had a bomb on my person! I hoped my brain would soon make this sound disappear although, someone who has had the op, said he doesn’t mind as it reassures him he’s still alive!

I told the surgeon I’d been exercising on a static bike since Simon, the cardiologist, had told me I needed a new valve. I wanted to get fit for surgery and had limited my heart rate to just 130 per minute and felt ok. He immediately told me to not do that again, to limit my exercise to just walking and my heart rate to no more than 100. He warned me of the grave danger of a sudden death from worsening the ventricular hypertrophy. My partner heard that loud and clear, so no cycling, swimming, heavy lifting, or heavy petting! I would be limited to slowly walking the dog. It also meant no foreign holiday – no-one would insure such a risk, until the valve was fixed. I couldn’t play football with the boys or go cycling with them. Having an arrhythmia whilst swimming isn’t great either for long term survival so ruled that out too. I wasn’t aware of how physically limited I was until I found Julien Roux’s Heart Alarm app for Garmin watches. He’d written the software for his father who also had aortic stenosis. Once I’d switched an alarm on to tell me when my heart rate reached 100 I was shocked at how often it was happening with minimal exertion. It was tens of times each day, with minimal exertion.
The surgeon warned me I might get admitted with chest pain, palpitations or a collapse whilst I was waiting and that would get me bumped up the queue, because the condition was becoming more critical. I realised that the twinges of pain I’d been having in my chest were angina, due to a lack of blood and oxygen getting to the heart itself, and the breathlessness was because my heart couldn’t pump out the body’s needs fast enough. No wonder I seemed unfit when skiing. It wasn’t so much physically unfit through lack of training, I was medically unfit. Even walking the dog up a slight slope or too quickly would trigger the alarm as would going up the stairs and even doing anything too quickly – sweeping up, showering, tying my shoe laces! Over time I got fed up with the alarm going off and got into the bad habit of muting it and not looking at the rate. Thinking about the risk of doing that though made me realise in fact, the alarm was a warning. The more I over did it, the more I’d be stimulating my heart muscle to get beefier and the more likely it was to trigger a fatal arrhythmia. I had to take notice of it and I had to slow down.
I am now one week away from a third attempt at an admission. The two previous times were aborted, one a couple of weeks before the admission date and one, after I’d arrived at the hospital, with my bag all psyched up for the real deal the following day. The NHS is massively under-resourced for what it is expected to do. Each time I was cancelled it was because other people more seriously ill than I needed treatment first.
I’m sure I’ll survive one more week and be able to write about the surgery, the aftermath and the recovery. Here’s hoping!
Shaun O’Connell, August 2023
With thanks to AL for his detail in editing. Any remaining errors are all mine!
If you liked this or if it helped you, please consider buying me a coffee!

[1] https://www.bhf.org.uk/what-we-do/news-from-the-bhf/news-archive/2023/july/heart-care-waiting-list-at-new-record-high accessed 7/8/23

Wow Sean what a fantastic article.
From a fellow participant of valve surgery.♥️
LikeLiked by 1 person
Very interesting
LikeLiked by 1 person
Do they not do TAVR procedures in the UK? I know someone in the US who just got one for aortic stenosis, and it’s a lot less invasive than open-heart surgery, has a much quicker recovery, and no warfarin. It also uses bovine tissue, so no metal clicking sound.
LikeLike
They do but I believe they are used primarily for patients who are older and are less able to tolerate open heart surgery. My understanding is that bovine valves do not last so long and need replacing after a decade or so. I’m hoping my On-X valve will outlast the rest of me!
LikeLike
Hi Shaun – I have a tissue valve now on its 12th year: wish me luck!
LikeLike
Best of luck Shaun, I hope all goes well and soon!
LikeLike
Many thanks Ian
LikeLike
Hi Shaun
Just wondering how your opera went and how your recovery is going.
Sending best wishes for a speedy recovery
LikeLike
Thanks Cath. Part 2 – the op and recovery are in drafting, at last! It’s all gone well.
LikeLike